This webpage is intended for UK HCPs only. Contains promotional material developed and funded by AstraZeneca. Prescribing information and adverse event reporting information is found at the bottom of the page.

Lokelma is indicated for the treatment of hyperkalaemia in a adult patients.1
starting as early as 1 hour1,2
in an 11-month study1,3
as seen in >1,700 patients across clinical trials1
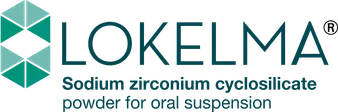
Although KDIGO and ESC guidelines position RAASi dose reduction and cessation as a last resort, down-titration or discontinuation of RAASi therapy is common following a hyperkalaemia event.
§Based on a retrospective analysis of a US electronic health record database (N>200,000) of patients ≥5 years of age with at least one outpatient RAASi prescription and at least two serum K+ readings.
RAASi included angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, a direct renin inhibitor and select mineralocorticoid receptor antagonists. RAASi dose level was defined as: maximum - labelled dose; downtitration - sub‑maximum dose of any RAASi lower than the labelled dose; discontinued - absence of RAASi prescriptions for >390 days subsequent to prior prescription. Median study follow‑up was 3.4 years.4
In advanced CKD: the mortality rate was 9.8% in patients on the maximum RAASi dose versus 20.3% and 22.4% in those who were on a submaximal dose or had discontinued therapy, respectively.4
In HF: the mortality rate was 13.7% in patients on the maximum RAASi dose versus 27.7% and 30.1% in those who were on a submaximal dose or had discontinued therapy, respectively.4
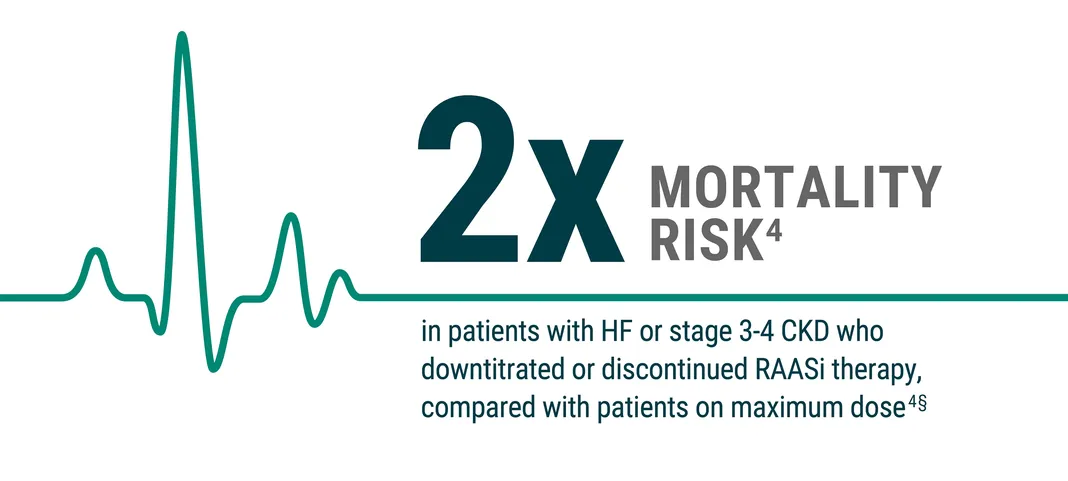
HARMONIZE was a phase III, randomised, double blind, placebo-controlled study evaluating the efficacy and safety of zirconium cyclosilicate for 28 days in outpatients with hyperkalaemia2,3
Please note that the recommended starting dose for maintenance therapy for non-dialysis patients with LOKELMA is 5 g once daily, which may be titrated to 10 g once daily as needed. No more than 10 g once daily should be used for maintenance therapy for non- dialysis patients. The 5 g once-daily dose can be down-titrated to 5 g every other day.
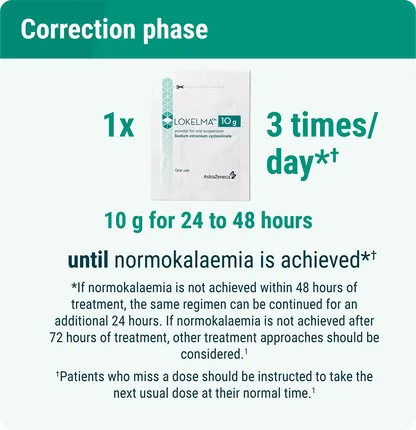
Open-label phase: LOKELMA 10g three times daily (n=258) administered for 48 hours, at which time patients (n=237) with normokalaemia (3.5–5.0mmol/L) were randomised to LOKELMA or placebo once daily.
Note: Normokalaemia defined as serum K+ 3.5-5.0 mmol/L and patients on dialysis were excluded from these studies.2,3 Error bars indicate 95% CI.
aP<0.001 vs. baseline;1 bIf a patient’s K+ value was between 3.0-3.4 mmol/L at any time during the randomised phase, the dose was reduced from QD to QOD for the remainder of the study;1 cP<0.001 vs. placebo during days 8-29;1 dThe extended maintenance group contained a small proportion of patients who were treated with LOKELMA unlicensed dose once daily.2

Patients were evaluated in clinical trials to establish LOKELMA safety profile; 507 patients received LOKELMA in a 12 month study

Pof patients reported oedema that was generally mild to moderate in severityb
of patients reported hypokalaemia (serum K+ less than 3.5 mmol/L) that resolved with LOKELMA dose adjustment or discontinuation
Constipation is also a commonly reported adverse reaction

LOKELMA does not affect serum Ca2+ or Mg2+ concentrations or urinary Na+ excretion

LOKELMA is not absorbed or metabolised by the body and there are no expected effects of other medicinal products on the pharmacologic action of LOKELMA

LOKELMA can transiently increase gastric pH and should be administered at least 2 hours before or 2 hours after oral medications with clinically meaningful gastric pH dependent bioavailability

Serum K+ levels should be monitored regularly during treatment. Monitoring frequency will depend upon a variety of factors including other medicinal products, progression of chronic kidney disease and dietary potassium intake. If severe hyperkalaemia should occur, LOKELMA should be discontinued and the patient re-evaluated. Refer to the Summary of Product Characteristics for more information including examples of such medicines.1